By Sofia Dewey, Intern at the AIDS Funding Collaborative
For more than a decade, the Affordable Care Act (ACA) and Medicaid expansion have served as vital lifelines for necessary healthcare for low-income adults — especially those living with HIV/AIDS.
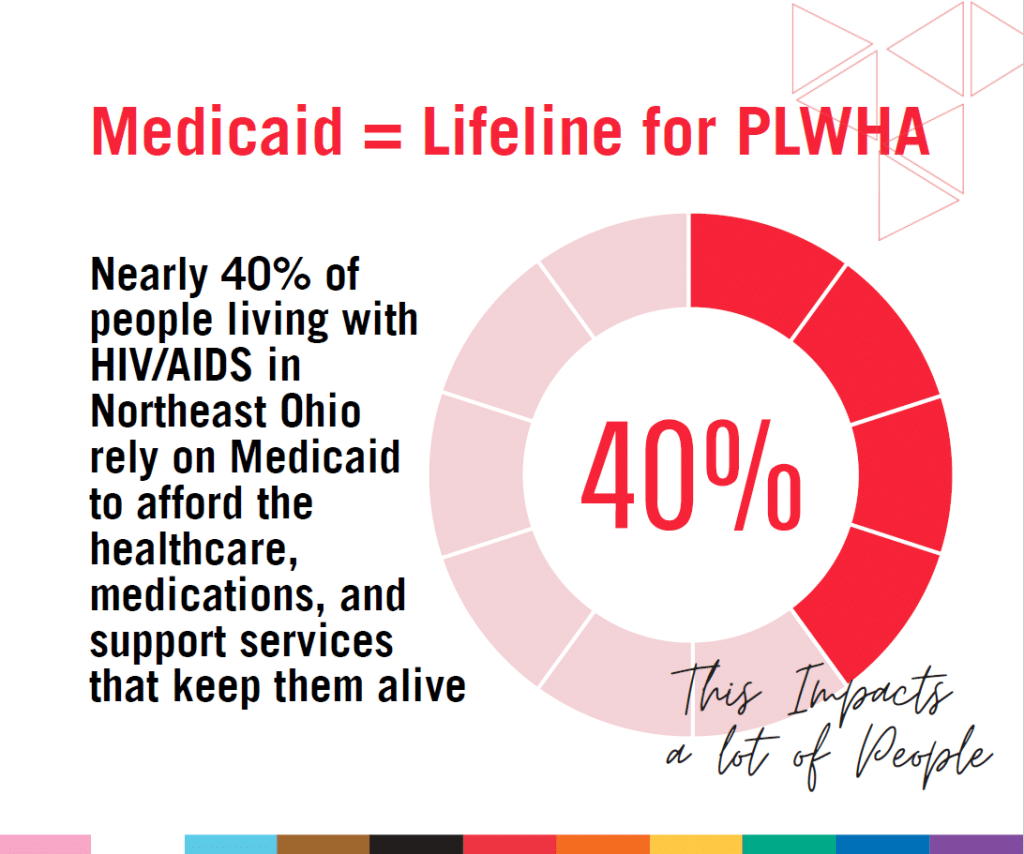
Forty percent of Americans living with HIV/AIDS rely on Medicaid.
However, proposed work requirements, restrictive federal policies, and administrative burdens threaten to unravel these gains, and new policy shifts risk creating a fragmented and increasingly inaccessible healthcare system for people living with HIV.
Community-based resources are critical safety nets — but they cannot replace the broad access Medicaid provides. Emergency financial assistance, reallocated public funding, and targeted outreach will be essential to help prevent people from falling through the cracks.
These policy changes won’t take effect overnight, but preparation is essential to ensure that people living with HIV remain connected to the care, treatment, and support they need to live long and healthy lives.
Medicaid expansion in Ohio
Before 2010, Medicaid coverage in Ohio was limited.
It included children in families with income at or below 200 percent of the federal poverty level (FPL) and parents at or below 90 percent, with few coverage options for adults aged 19–64 who didn’t have access to employer-sponsored coverage.
The FPL is a federal income measure used to determine eligibility for public programs; for a single person in 2025, 100 percent FPL is about $15,000 a year.
The ACA created the Health Insurance Marketplace, a centralized federal platform where people earning between 100-400 percent FPL could compare insurance plans and access tax credits, opening new opportunities for people with HIV/AIDS to secure and maintain affordable healthcare.
Since Ohio expanded Medicaid in 2014, hundreds of thousands of low-income residents have gained access to care. Medicaid expansion made adults under age 65 with incomes up to 138 percent FPL eligible for coverage.
As of May 2025, around 770,000 Ohioans were enrolled in Medicaid. In Cleveland, about 45 percent of residents rely on Medicaid for their healthcare needs.
Forty percent of Americans living with HIV/AIDS rely on Medicaid for comprehensive and affordable healthcare. Medicaid is the largest source of federal funding for HIV-related health care, covering chronic conditions, mental health care, and essential treatment. Black residents — who represent 58 percent of Medicaid enrollees in Cleveland and 57 percent of HIV cases — particularly benefit.
The 2025 Cleveland Health Survey found no significant differences between Medicaid and private insurance recipients in routine care access, mental health services, or delaying care due to cost. This is a significant finding, given that Medicaid enrollees often face greater social and financial insecurity.
These gains are now at risk.
In states that have expanded Medicaid, like Ohio, adults earning up to 138 percent FPL qualify for Medicaid.
In contrast, the states that have not opted in to expansion – non-expansion states – leave an estimated 1.5 million adults in a “coverage gap,” earning too little for subsidies (only available starting at 100% FPL, but not below) but too much for Medicaid.
Impact on the Ryan White HIV/AIDS Program
Named after Ryan White, the Indiana teenager who faced discrimination and stood up to HIV stigma, the Ryan White HIV/AIDS Program funds essential medical care and support services for low-income individuals with HIV.
As a “payer of last resort,” Ryan White funds are used after all other coverage options are exhausted. Since the ACA’s implementation, Ryan White has expanded its support — offering not only treatment but also supportive or wraparound services that help people stay in care.
- Part A serves eligible metropolitan areas with high HIV burdens, funding both medical and support services. Community-driven Planning Councils in these areas (like the one in Cuyahoga and 5 surrounding counties) ensure that services reflect the needs of local populations, including people with HIV.
- Part B provides grants to states and territories, including funding for the AIDS Drug Assistance Program (ADAP), which supplies medications and covers insurance premiums and co-pays.
In Ohio, the ADAP program (OHDAP), primarily funded by Ryan White Part B, covers residents earning up to 500% FPL. In 2023, 66 percent of ADAP clients earned at or below 200 percent FPL, and 41 percent were at or below 100 percent FPL.
ADAPs will not be able to absorb all the unmet needs resulting from Medicaid losses and cannot cover care for non-HIV-related conditions, leaving people without coverage for co-occurring conditions.
Work requirement
Further complicating the landscape for Ohioans living with HIV, the Ohio Department of Medicaid (ODM) has submitted a plan to the federal government to implement work requirements for Medicaid expansion enrollees.
The recent federal reconciliation bill, or H.R. 1, includes a work requirement for all Medicaid expansion enrollees, and it is still unknown exactly how the state and federal work requirement policies will interact.
Ohio’s submitted plan says that to remain eligible for expansion, one must be at least 55, employed, enrolled in education or treatment programs, or have a serious medical or mental health condition.
“Employment” is broadly defined to include unpaid caregiving, volunteering, internships, community service, or receiving unemployment.
Additionally, the reconciliation bill also places a federal prohibition on enforcing federal nurse staffing requirements in long-term care facilities, which will affect aging people living with HIV.
If approved, these requirements will remain in effect unless overridden by stricter federal mandates set for December 2026.
450,000 Ohioans at risk
While Ohio doesn’t have a traditional coverage gap, as non-expansion states do, this new policy is poised to create one.
A new coverage gap will emerge for those earning between 0-100 percent FPL as they’ll be Medicaid-eligible but not enrolled, and not subsidy-eligible, since subsidies don’t kick in until 100 percent of FPL.
ODM estimates around 62,000 people will lose eligibility, though this number doesn’t include those not currently working. Inclusive estimates place around 450,000 Ohioans at risk.
For people with HIV, these rules could delay diagnosis, disrupt care, and jeopardize viral suppression — especially during gaps in insurance verification at application and renewal (which will now require a one-month look-back every six months).
This creates serious barriers for people newly diagnosed with HIV and threatens to reduce care access, quality and continuity of care for Ohioans living with HIV.
By undermining enrollment, continuity of care, and quality standards, they threaten to reverse decades of gains in health equity and HIV treatment outcomes. 🔥
Ignite action
- To learn more about the AIDS Funding Collaborative, click here.
- Check out the Accountability August action alert toolkit from #SaveHIVFunding here.
- To find a doctor that prescribes HIV PrEP near you, click here.
- To find a Ryan White HIV/AIDS Program medical provider in your area, click here.
- If you are a young LGBTQ+ person in crisis, please contact the Trevor Project: 866-4-U-Trevor.
- If you are an transgender adult in need of immediate help, contact the National Trans Lifeline: 877-565-8860
Know an LGBTQ+ Ohio story we should cover? TELL US!
Submit a story!